False Claims Act Impact On Medical Billing and Coding
Posted on December 26th, 2023 / Under Medical Billing / With No Comments
Initially, the False Claims Act in healthcare was enacted during the Civil wall to impose liability on individuals and organizations defrauding the government. This is why FCA is also known as Lincoln Law.
Since then, the False Claims Act has covered healthcare fraud and massively impacted medical billing and coding processes. Fraudulent billing practices lead to compliance issues, legal penalties, and improper reimbursement, so FCA is a critical deterrent for such practices.
Keep reading to learn about the False Claims Act in healthcare and the spectrum of fraudulent healthcare activities it addresses.
Understanding the False Claims Act
Medical billing and coding processes are highly complex, which is one reason these processes are vulnerable to intentional fraud and errors. For instance, submitting a claim for medical services that are deemed unnecessary or non-existent is a common intentional fraudulent activity that is covered under the False Claims Act.
A healthcare provider’s billing practices are governed under the False Claims Act once they contract with the state or federal government to treat Medicare beneficiaries. Under this contract, all medical claims are submitted to Medicare. In case of healthcare fraud, like unnecessary services, neglect, use of faulty equipment, and inadequate services, healthcare providers are liable for civil and criminal penalties. To avoid such penalties, providers must ensure billing and claim submission is accurate and compliant with healthcare regulations.
If reckless disregard or intentional misconduct of a provider is established, Medicare can directly sue them in civil court. It is crucial to note that the court can impose liability without finding the provider’s specific intent to defraud.
The mere submission of a false claim to Medicare is considered a clear violation, irrelevant to the payment status of the claim. In 2021, healthcare fraud accounted for over $5 billion of the total $5.6 billion Department of Justice’s False Claims Act’s settlements and judgments.
Some Federal False Claims Act examples are:
- Intentionally present a false claim or cause it to be present to obtain payment from the federal government.
- Defraud the government by getting a false claim approved or paid.
- Create, use, or influence the creation of a false statement or record for reimbursement.
- Create, cause to be created, or intentionally use a false document, record, or statement to decrease, completely avoid, or conceal the obligation to pay or transmit property to the government.
Difference Between Billing Fraud and Abuse
Fraud
In billing, fraud is defined as the act of willfully planning or executing a scheme to defraud the federal government and obtain income from healthcare programs such as Medicare. Fraud is attempted through fraudulent representations or any payment or property that is under the custody of the healthcare benefit program.
Examples of billing fraud include:
- Billing for more services than the patient received.
- Billing for premium medical equipment while substituting standard or faulty equipment during treatment.
- Misrepresentation of the date of service to justify higher reimbursement.
- Inconsistent medical documentation submitted with a billed service.
- Gaining duplicate payments through double billing.
Abuse
Billing abuse is not always intentional, but if it becomes consistent, it can be termed as healthcare fraud. It is defined as a provider or contractor’s behavior or conduct that is inconsistent and contradicts the standards of any business, medical practice, or insurance company.
Examples of billing abuse include:
- Waiving co-pays or co-insurance to encourage the patient to obtain further treatment.
- Billing from an out-of-network location while requesting pre-authorization under the network’s location.
- Conducting experimental services that do not meet a specific standard.
- Exaggerating or misrepresenting a diagnosis.
- Not disclosing discounts or hidden payments beforehand.
How False Claim Act Is Brought
The False Claim Act comes into play under two circumstances. One is when a former or current employee of a medical practice, with adequate knowledge of internal fraudulent activities being performed in the practice, files a lawsuit on behalf of the government.
They can also be called a whistleblower or relator in this scenario. Whistleblowers can be awarded around 10 to 30 percent of the total amount recovered in the lawsuit for filing the qui tam claim.
On the other hand, the U.S. Department of Justice can also file a False Claim Act if they have information on false claims being submitted by a practice. The DOJ also files claims for fraudulent healthcare practices when they learn about them through another local, state, or federal agency.
Penalties for Violating the False Claims Act
If a provider or healthcare facility violates the False Claims Act, the penalties can include:
- Repayments: Under the court’s order, the provider or medical practice can be ordered to make repayments to the healthcare benefit program such as Medicare, Medicaid, or Tricare.
- Corporate Integrity Agreements: When a provider, organization, or entity enters a corporate integrity agreement, they must meet specific criteria before being able to bill a federal agency for the services they provide.
- Treble Damages: Healthcare providers that make illegal self-referrals or kickbacks, billing Medicare a total of $1 million, can be sued and court-ordered to pay $3 million in damages.
- Statutory Penalties: A single False Claims Act violation is worth $11,000 in damages. So, if a provider violates the Act once, they can be legally required to pay $11,000 in damages.
FAQs
What is an example of False Claims Act Healthcare?
A common False Claims Act violation committed in the healthcare industry is upcoding, where the hospital assigns codes of expensive services to standard or inexpensive services provided to the patient. This is done to increase reimbursement obtained from Medicare.
How does the False Claims Act affect medical billing?
False Claims Act impacts a healthcare organization’s billing practices by deterring fraudulent activities. Providers that engage in improper billing will be subject to legal repercussions, including hefty fines and exclusions from healthcare benefit programs.
Why does the False Claims Act matter to healthcare providers?
The False Claims Act enables the federal government to bring lawsuits against healthcare providers engaging in billing abuse or fraud, promoting ethical billing practices in the healthcare industry.
Read More...Role of Encounter Forms in Provider Records and Billing
Posted on December 22nd, 2023 / Under Medical Billing / With No Comments
On average, a doctor works around 51.4 hours a week, seeing around 11-20 patients a day. With these numbers, it’s challenging for hospitals to efficiently keep track of patient information without proper staff or encounter forms.
Comprehensive and organized medical records are the cornerstone of effective management of a healthcare facility and delivering high-quality care.
Encounter forms have become more crucial for billing ever since the digitization of medical records. Encounter forms systematically encapsulate information about billable treatments, making the medical billing process more seamless.
Keep reading to explore further the role of encounter forms in patient-provider relationships and billing.
What Is a Superbill or Encounter Form?
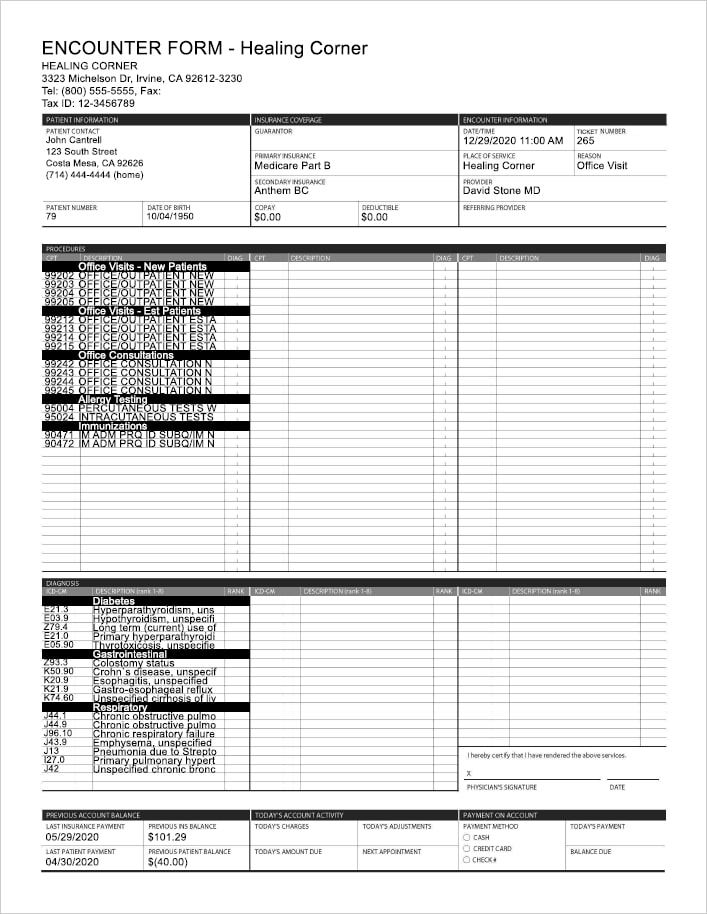
Encounter forms or superbills are documents containing comprehensive summaries of patient encounters, diagnoses and procedural codes, and treatments performed. In short, these forms withhold the insights of each interaction between a healthcare provider and a patient.
This standardized information streamlines the billing and reimbursement cycle through timely and accurate claim submission. Encounter forms also contain insurance and patient demographics.
Here are some things included in superbills.
- Basic patient information, including patient identification number.
- Demographic information like occupation and ethnicity.
- List of physicians assigned to the patient’s case.
- The reason behind the patient’s visit.
- Past medical history of the patient.
- Detailed information about the patient’s current illness, the onset, duration, and progression of the illness.
- The complexity of visits and assigned procedural and diagnosis codes.
- Staff and provider signatures indicating approval of the encounter form or superbill.
Examples of Encounter Forms
The layout and formats of encounter forms differ depending on the specific needs of the facility and the nature of the medical case. For example, dental care encounter forms include information like x-ray results, oral examination findings, dental history, treatment plans, and follow-up care.
Other examples of encounter forms include specialty-specific encounter forms, such as cardiology or neurology forms, gyne encounter forms, psychiatric encounter forms, pediatric superbills, and primary care encounter forms.
These examples will help you thoroughly understand what is an encounter form. It is crucial to record accurate information on superbills for effective treatment planning and preventing billing errors.
Importance of Encounter Forms In Billing
The information present in an encounter form is critical for multiple purposes. For instance, superbills enhance communication and collaboration among the healthcare staff as well as between the patient and provider.
With essential information regarding the patient’s condition being readily available, any changes in the treatment plans and further specialist recommendations can be conveyed easily.
Comprehensive documentation, such as patient encounter forms, allows healthcare organizations to maintain consistent and thorough patient records.
Information relevant to reimbursement and billing is also included in medical encounter forms. The standardized format used in patient encounter forms makes it easier to record medical diagnoses and services and translate them into codes. This contributes to coding compliance.
Due to encounter forms, claims can be submitted on time, preventing delayed or denied reimbursements. These documented records also assist healthcare facilities in legal inquiries and audits and ensure the facility is compliant with healthcare regulations.
All facilities use electronic encounter forms for their patients because manually filling in the form and adding signatures to approve each form increases the administrative burden on the hospital’s staff.
With digitized encounter forms or superbills, providers have more time to focus on providing high-quality care to their patients. Another way encounter forms improve the quality of patient care is by allowing providers to identify and eliminate any negative patterns and outcomes documented in previous forms.
Hospitals can encounter liability issues now and then, and without detailed records of patient encounters, it can be difficult to mitigate the risk of legal penalties. With complete information on recommendations made and treatments administered to the patient, providers and healthcare facilities can avoid potential liability claims.
FAQs
What are the key components of Superbills/ Encounter Forms in medical billing?
The content recorded in superbills or encounter forms can differ by each patient encounter, but some key components of these forms include ICD-10 and CPT codes, modifiers, tracking units of services, patient demographics, medical history, breakdown of services provided to patients, and provider details.
Information needed on a comprehensive Superbills includes?
If you’re wondering in what format a superbill comes, you should know that comprehensive superbills include insurance coverage information, patient instructions, fee schedules, and quantity and units or rendered procedures, along with basic patient information, medical history, translation of services into billable codes, and provider information.
4 Examples of Superbills in Healthcare?
Superbills are defined as detailed invoices outlining services rendered to patients. There are different types of superbills detailing specific information. Some examples of superbills include dermatology and dermatology practices. These superbills include dermatologic procedures, dates of service, patient data, and any corresponding codes. Other examples include primary care superbill, orthopedic superbill, and gynecology superbill.
Read More...Free Standing Emergency Rooms Billing Services And Your Need To Outsource
Posted on December 21st, 2023 / Under Medical Billing / With No Comments
Freestanding ER may be a new trend in the healthcare industry, but they have been around for ages. The purpose of freestanding emergency departments is to provide emergency care beyond the four walls of a healthcare facility.
Emergency room billing is a major contribution to a hospital’s total workload, and managing patient care and physician billing duties can be hectic and challenging. This is why most organizations outsource this aspect, saving them time and money.
However, outsourcing emergency room billing is not as straightforward as it seems. Let’s take a look at the challenges and benefits of outsourcing free standing er billing.
Understanding Freestanding ER
Freestanding emergency rooms are standalone ERs that are not connected or in the locality of a hospital. However, they are owned by a hospital or an organization.
Having been around for nearly 50 years now, these freestanding emergency departments are easily accessible in communities.
To ensure the highest quality of patient care, freestanding emergency departments are equipped with advanced and innovative medical technologies. FSERs are also staffed by highly skilled providers, including trained paramedics, nurses, physicians, and other support staff.
Since these departments are designed to handle a diverse array of medical cases effectively, patients who visit freestanding emergency rooms can expect a high level of patient care to be delivered.
However, patients must remember that these freestanding emergency rooms may have distinct billing practices. For instance, most Freestanding ERs may not be directly affiliated with most insurance networks.
Awareness of any insurance implications and services provided can help patients make informed decisions when seeking medical assistance in a freestanding emergency room.
Differences Between Hospital ERs and Freestanding ERs
To fully understand what is a freestanding emergency room, you should learn about some differences between hospital emergency rooms and freestanding ERs.
While both ERs are open around the clock, seven days a week, one notable difference is the geographic location.
Hospital ERs are generally located in urban areas, mainly in general hospitals, which can be inaccessible to certain communities. However, freestanding ERs are strategically placed in areas where they can be accessible to communities.
Another difference is that patients have access to a wide range of specialists when seeking medical assistance in a hospital ER, but that might not be the case in a freestanding ER, although patients receive comprehensive care in both facilities.
FSERs have short wait times compared to hospital ERs, and their billing practices can also vary. Hospital ER billing is generally integrated with the hospital billing system.
Common Issues With Outsourcing Freestanding ER Billing
Here are some common issues with outsourcing free standing ER billing:
Privacy Concerns: Sensitive patient information must be kept confidential according to HIPAA regulations. Healthcare providers must partner with outsourcing billing services with robust security measures.
Hidden Fees: Some outsourcing billing partners may impose hidden fees once you enter a contract. Ensure that you research thoroughly and partner with a billing service that helps you minimize operational costs.
Slow Response Time: Slow response time from your outsourcing billing partner can have severe financial implications. Timely billing is critical for maintaining cash flow.
Benefits of Outsourcing Freestanding Emergency Room Billing
While there are certain drawbacks of outsourcing freestanding emergency room billing, the advantages of doing so outweigh the issues.
Let’s dive into the benefits of outsourcing ER billing for healthcare organizations.
Reduced Administrative Burden
Outsourcing is a great way for healthcare providers to offload some billing responsibilities, including claim submission, payment posting, and following up on claim status.
All of the organization’s resources can be focused on more practical objectives by outsourcing freestanding emergency billing, including investing time and effort in more patient-focused activities.
Fewer Billing and Coding Errors
Billing and coding errors can be a major concern for any healthcare organization, causing the internal staff and providers to divide their attention between providing high-quality patient care and addressing billing issues.
Outsourcing medical billing for your freestanding emergency department to qualified medical billers will ensure billing is performed in compliance with current industry laws and with the help of technological advancement.
This would improve the overall accuracy of billing processes and reduce claim denials.
Improved Cash Flow
Improved cash flow is one of the biggest benefits of outsourcing freestanding ER billing. For one, it can help you avoid a significant backlog created by not developing and submitting medical claims on time.
When the claims are filed and developed on time, it will improve cash flow. Consistent cash flow results in improved income streams for the facility.
Patient Satisfaction
Delivering high-quality patient care is the primary goal of every healthcare facility. By outsourcing your freestanding ER billing practices, providers can give patients their undivided attention, improving patient satisfaction.
Mitigating Compliance Risks
Healthcare facilities need to stay updated on coding requirements to reduce coding errors. Errors in coding can not only be costly but also result in severe legal penalties.
However, if you outsource billing and coding of your freestanding ER department, coding and billing experts well-versed in coding and other healthcare regulations will perform accurate coding, helping you avoid legal repercussions and mitigating compliance risks.
FAQs
What is a freestanding ER room?
Freestanding ER departments provide patients with emergency care similar to hospital ERs, but they are not located inside or attached to a hospital. Instead, they are located close to communities to make ER services accessible to patients. Freestanding ER departments are open throughout the day, unlike urgent care centers.
Are stand-alone ERs more expensive?
While the cost of care depends on the type of procedures and services rendered to a patient, freestanding or stand-alone ERs can be more expensive than hospital ERs.
Read More...Physician Credentialing Importance In Healthcare Improvement
Posted on December 19th, 2023 / Under Medical Billing / With No Comments
According to a recent survey, 26% of physicians state that patients can be potentially protected against malpractice and other medical errors with the help of physician credentialing.
Medical or provider credentialing extends beyond the assessment of a provider’s academic achievements, it encompasses a comprehensive evaluation of their experience, clinical skills, and ethical standing.
Credentialing in medical billing is a challenging task, and to make it accountable and steer clear of potential mistakes, here is what you need to know.
Overview of Physician Credentialing
To put it in simpler terms, credentialing in medical billing is a process through which healthcare facilities evaluate the eligibility of prospective practitioners.
The process involves validating physicians’ certifications and licenses, confirming their work history and malpractice coverage, and assessing their education and training.
The legal authority of staff selection and overseeing the credentialing process lies with the official board of a hospital.
Not just that, insurance providers and other healthcare facilities also utilize the medical credentialing process to verify healthcare providers including therapists, pharmacists, dentists, nurses, and physicians.
Each time a healthcare provider switches specialties or opens a new practice, they must undergo credentialing. Physician credentialing services ensure that patients receive care from healthcare providers that meet certain standards of professionalism.
How Does It Work?
So, exactly does provider credentialing work? It involves three stages: credentialing, privileging, and enrollment or contracting.
Many people tend to confuse credentialing with privileging, which is an entirely different process.
While medical billing credentialing is the evaluation of a doctor’s qualifications, privileging done at healthcare facilities and hospitals provides credentialed physicians with the authority to perform specific procedures. For example, a physician granted privilege by the hospital can perform procedures like endoscopy.
Privileging is granted by conducting OPPE (Ongoing Professional Practice Evaluation) and FPPE, which is a more focused evaluation conducted only if there are concerns related to the physician’s practice.
This step comes after credentialing in the provider credentialing process. The third step is contracting in physician medical billing. This entails the involvement of payers and insurance companies.
In this step, physicians apply for participation in health insurance networks. After approval, the physician enters a legal agreement in which specific terms and reimbursement rates are settled, allowing physicians to bill for their services.
If you’re confused about how to get credentialed with insurance companies, here are some steps you can follow:
- Researching potential insurance providers.
- Gathering mandatory documentation.
- Filing a Council of Affordable Quality Healthcare application for a provider identifier.
- Follow-ups and re-credentialing.
Re-Credentialing
Appropriate credentials are crucial for providers to perform treatment and get reimbursement. And if a provider has been credentialed, the process does not stop there.
The medical industry is continuously evolving, and to meet certain criteria, providers undergo re-enrollment or re-credentialing every two years or so.
Once the credentials expire, providers receive a letter entailing a re-credentialing deadline. Repetition of the same credentialing process by a medical credentialing specialist ensures that the provider’s skills are up to par.
Importance and Significant Benefits of Credentialing In Healthcare
After knowing what credentialing is in healthcare, you may still be wondering why it’s important.
Let’s dive right into how credentialing is directly linked to healthcare improvement.
- Avoiding Lawsuits: It’s not uncommon for healthcare organizations to confront false claims and lawsuits. When that happens, credentialing can help protect the organization and its providers.
- Safeguarding Patient Wellbeing: Patient safety is one of the primary objectives of provider credentialing. Any issues in the provider’s work history are uncovered during the credentialing process.
- Building a Reputation In the Industry: Medical credentialing also plays a critical role in preserving and shaping the reputation of a healthcare facility as it validates the qualifications of healthcare providers.
- Prevents Loss of Revenue: Proper physician credentialing reduces delayed reimbursements, preventing thousands of dollars worth of loss in revenue of a medical practice.
- Access to Patient Bases: Credentialing allows practices to boost their revenue streams by accessing more patient bases, such as patients covered under health insurance.
- Delivering a Competitive Edge: Qualified practitioners are more inclined to join credentialed facilities and similarly, you can enlist professional and highly skilled providers in your practice through medical billing credentialing.
Common Physician Credentialing Mistakes
Allocating adequate resources to properly credential each provider can be a hassle most organizations are not equipped for. Extremely lengthy credentialing processes are one of the basic causes of provider credentialing mistakes.
With that said, here are some common credentialing mistakes on the provider’s end.
- Providing inaccurate or outdated information during credentialing.
- No follow-ups on re-credentialing and failure to respond to requests for additional documentation.
- Submitting expired credentials.
- Not disclosing issues about former work history, such as malpractice.
- Failure to track expiration dates of licenses and certificates.
On the other hand, there are also common credentialing mistakes on the staff’s end that can lead to errors.
- Inaccurate data entry can lead to confusion.
- Delaying provider credentials and not acquiring provider credentialing services.
- Allowing providers to practice and perform treatments before credentialing is complete.
- Relying on manual workflow instead of automating the credentialing process.
- Not using primary source verification to avoid errors.
FAQs
What are the provider credentialing process steps?
The provider credentialing steps include researching documentation requirements, selecting insurance providers, ensuring the accuracy of the information, completing the CAQH, waiting for the insurer’s approval, follow-up, and re-certification.
What makes credentialing in medical billing essential?
Credentialing in medical billing is essential for numerous reasons, including reduction in medical errors, streamlining the reimbursement process, compliance, maintaining professionalism, and maintaining patients’ confidence in the providers treating them.
Read More...Medicare 8 minute Rule Billing: Also Known As Direct Time CPT Codes
Posted on November 30th, 2023 / Under Medical Billing / With No Comments
Underbilling is a serious issue in the healthcare industry, and one primary cause is the providers’ lack of knowledge regarding Medicare rules. One commonly understudied Medicare rule is the 8 minute rule.
At first glance, the Medicare 8 minute rule seems fairly straightforward; treatments are billed to Medicare in units, and treatment must last no less than 8 minutes for a unit to be billed to Medicare.
Unfortunately, oversight in this regard could lead to mistakes, resulting in problems like incorrect billing, underpayment, or delayed reimbursement.
As a provider, here is how to avoid mistakes when using the 8 minute rule units to bill Medicare.
Understanding the 8-minute Rule in Billing
As established earlier, to receive payment from Medicare for some CPT codes, a provider should provide direct treatment to a patient for a minimum of 8 minutes.
Any service, specifically outpatient therapy services like physical or occupational therapy, that lasts less than 8 minutes in duration, cannot be billed to Medicare. This rule also only applies to time-based CPT codes.
It’s also crucial to understand that only certain services fall under this rule, such as Medicare Part B services. It also applies to payers who follow Medicare billing guidelines; in addition, the 8-minute rule only applies when the service is performed in person.
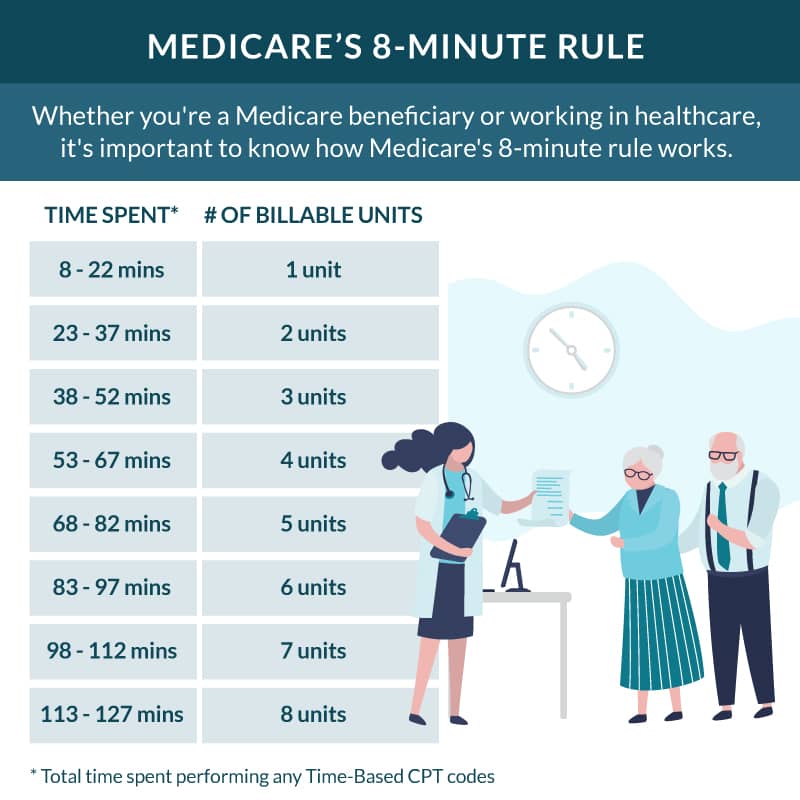
Services covered by the Medicare 8 minute rule are billed in 15 units.
For example, if a service lasts anywhere between 8 to 22 minutes, it would be billed in a single unit. But if the service takes more than 22 minutes, such as 37 minutes, Medicare will be billed 2 units for each 15-minute interval and so on. You can review the Medicare 8 minute rule chart for a clear understanding of billable units.
However, any services that last less than 8 minutes may not be separately billable. In case a patient is provided more than one service or procedure in a single minute, Medicare would review the combined minutes of each service. If the combined minutes pass the minimum threshold of 8 minutes, Medicare can be billed separately for each type of service.
The CMS 8 minute rule applies to outpatient service providers, including hospital outpatient departments, private physical therapy clinics, rehabilitation facilities, occupational therapy clinics, nursing facilities, and speech-language pathology centers.
Medicare rules, such as the AMA 8 minute rule, do not apply to non-medical insurance unless stated explicitly in their policies. That is because most private insurance companies don’t allow mixed remainders.
Mixed remainders are referred to as the leftover hours of a multiple-timed service that do not meet the minimum threshold. Mixed remainders from different services can be combined to meet the 8-minute threshold and be billed as units. Moreover, the 8-minute rule also applied to Medicaid services.
You can also refer to the 8 minute rule cheat sheet to understand the difference between billing for insurances that follow CMS guidelines and those that follow AMA guidelines.
Difference Between Time-Based CPT Codes and Service-Based CPT Codes
Service-based codes are generally untimed and billed as a single unit as they do not depend on the amount of time a service takes. Some common examples of service-based codes are E/M (Evaluation and Management) codes, procedures, and diagnostic tests. Service-based codes are reimbursed depending on the complexity of the service provided.
On the other hand, time-based codes are billed in 115 increments, depending on the amount of time spent on a service. There is also a set of rules that apply to make time-based codes billable. For example, the service provided should have been one-on-one for a time-based code to be reimbursed.
In some cases, time-based units and service-based units can be a part of the same treatment session, but they will still be billed separately.
Calculating Billable Units
Knowing how to calculate medical billing units is essential for claims scrubbing and submission. Here is how you can calculate billable units.
- Firstly, calculate the number of minutes spent on a service.
- Divide the total number with 15. This would give you the amount of billable units.
- Now, identify any leftover minutes. If there are multiple leftover minutes from different services, you will now have what is called a mixed remainder.
- If the mixed remainder is equal to or greater than half of the minimum threshold (which in this case would be 4 minutes), it can be rounded up to another billable unit.
Consider this example: if the total number of minutes you spent on a time-based service was 30, you can divide it by 15. This way, you will get two billable units.
Key Differences Between Rule of 8s and 8-minute Rule
Many people confuse the rule of 8s with the Medicare 8 minute rule when, in fact, the rule of 8s is the label used to describe the 8 minute rule in the CPT code manual. Typically, the rule of 8s is applied to non-medical insurance payers for Direct Time CPT Codes.
While the rule of 8s follows the same principles as the 8-minute rule, there is a bit of distinction. For instance, the rule of 8s requires practitioners to provide at least half of the service to bill for one unit.
8-minute Rule Mistakes to Avoid
It can be challenging to properly bill under the Medicare 8 minute rule for physical therapy.
There are often certain mistakes people make, like presuming they’ll be getting charged extra for services lasting longer than 8 minutes or believing that this rule applies to all types of services provided by their assigned physician.
Physicians should discuss the 8 minute rule with Medicare beneficiaries to alleviate their concerns and answer relevant queries.
On the provider end, to avoid any billing mistakes while using the 8 minute rule, you should,
- Accurately document the total time spent performing billable activities.
- Bill in correct increments. For instance, bill for three units if the total time spent on service is 52 minutes.
- Assign correct CPT codes to the services provided.
- Provide clear and concise documentation detailing the services provided to the patient and the patient’s response to the treatment.
- Train your healthcare staff on how to utilize the Medicare 8-minute rule properly.
FAQs
How many minutes are in a billing unit?
According to the 8-minute rule by Medicare, a billing unit typically equals 8 minutes of a physician’s time. So, if a physician performs a service that takes around 8 minutes, it will be billed as one unit.
8-minute rule importance in physical therapy?
The 8 minute rule guides physical therapy specialists on how to properly document their time during a patient encounter and perform accurate billing for reimbursement. Adhering to the 8 minute rule helps physical therapy clinics optimize revenue.
Read More...Medical Practice Management Software: Various Uses For Maximizing Healthcare Efficiency Including Billing Tasks
Posted on November 29th, 2023 / Under Medical Billing / With No Comments
People belonging to the healthcare industry, whether therapists, direct care practitioners, specialists, or chiropractors, all know that the realm of medical practice is extremely fast-paced.
Managing all operations from the front desk to the back office can be considerably challenging for healthcare organizations. But this is where a Medical Practice Management Software, also known as PMS, comes in.
The benefits a PMS brings to the table for a healthcare practice go beyond just organizing patient records, reporting, and appointment scheduling. In fact, it plays a much more pivotal role, streamlining some crucial operations, including billing tasks.
Let’s dive right in and learn the importance of cloud-based medical practice management software, its critical features, and its benefits.
Importance of PMS in Healthcare
Practice management involves both routine operational and financial tasks. Many large hospitals and healthcare organizations have professionals overlooking such tasks, but it’s often challenging for small and medium-sized healthcare practices to do the same.
So, instead of handling the administrative burden of keeping every operation organized on its own, small and medium-sized practices can invest in medical practice management software.
There are typically four main types of PMS, cloud-based medical practice management software, desktop-based PMS, client-server PMS, and on-premise PMS. To choose the right PMS for your practice, consider checking medical practice management software reviews.
Overall, a PMS can significantly contribute to the efficiency of a practice. Let’s break down the tasks a PMS can streamline for healthcare organizations.
- Keeping sensitive patient information protected against breaches.
- Automating appointment scheduling to reduce wait times.
- Recording and managing patient demographic information.
- Reducing the likelihood of errors in the medical billing process.
- Integration with payers to improve information exchange and streamline claims submission.
- Generating reports to facilitate audits.
Features of Medical Practice Management Software
Each PMS in the market comes with a distinct set of features, but let’s review some standard medical practice management software features you should look for.
1. Integration With Other Systems:
PMS can seamlessly integrate with other systems like EHR, EMR, and Telehealth functionalities. This type of integration improves the overall quality of patient care.
For instance, integration with an EHR (Electronic Health Records) system contributes to error reduction and provides easy access to patient information.
It also minimizes the need for manual data entry, allowing physicians to easily access and update patient information and make informed medical decisions.
Similarly, integration with Telehealth facilitates the continuum of care, allowing physicians to conduct virtual consultations and share electronic prescriptions with patients.
2. Streamlining Billing Processes:
Billing accuracy is fundamental for any medical practice, and it can be achieved with the help of PMS. The billing management feature allows you to make online payments and create and send invoices.
It also helps minimize the need for separate billing software by eliminating coding errors. This improves reimbursement rates and cuts down the administrative burden on the healthcare staff, allowing them to focus more on providing quality patient care.
3. Enhancing Patient Engagement With Patient Portal:
One practical feature of the medical practice management software is allowing patients to participate virtually in their healthcare journey.
Through patient portals, patients are able to access their test results, access medical records, and schedule appointments with their physicians. This increases patient satisfaction.
4. Resource Management:
The resource management feature allows practices to utilize the PMS to keep track of the inventory. Practices can also create and manage schedules for equipment maintenance and automate the process of reordering medical equipment.
5. Reporting:
Practice management tools allow you to generate reports on insurance claims, patient demographics, and much more. These reports allow practices to analyze financial and operational performance and make data-driven decisions.
Essential Benefits of Using PMS
• Reduced Administrative Burden:
With critical tasks like generating invoices, managing appointment schedules, bookkeeping, collecting patient demographics, and more just a single click away, a medical practice management system greatly reduces the administrative burden on the staff of a healthcare practice. This allows the providers and staff to avert their attention to the delivery of high-quality patient care.
• Minimizing Wait Time and No-Show Rates:
Automating appointment scheduling allows providers to organize the schedule and minimize any delays, reducing wait time during appointments. PMS that contain medical CRM functionalities allows practices to send appointment reminders to patients, minimizing no-show rates due to missed or forgotten appointments.
• Seamless Billing:
Medical practice management software eliminates the need for any paperwork for billing. Providers can keep track of all payments and invoices using PMS. This also expedites the claims submission process and reduces claim rejection rates.
• Data Centralization:
With financial, patient, billing, and insurance information accessible in a single software, billing specialists, healthcare providers, and the administrative staff can collaborate seamlessly. Data centralization ensures the personnel of a medical practice are on the same page.
• Effective Communication:
Not only does PMS improve communication between physicians and patients but also allows integration with systems present on the payers’ ends, streamlining the exchange of information between billers, coders, and payers.
• Improved Patient Care:
Improving patient care is the bottom line for any healthcare practice, and implementing medical practice management software is a gateway to improved patient care and satisfaction. PMS reduces errors in medication and diagnosis, fostering better clinical decisions and improving patient outcomes.
• Transparency:
With the accessibility of generating performance reports, practices are able to analyze them and identify areas that require improvement.
FAQs
What are the key features of Medical Practice Management Software?
All patient management software in the market are different in some aspects, but some key features of practice management software include billing, scheduling, coverage verification, business intelligence, and patient data management.
What is the difference between EHR EMR and Practice Management Software?
EHR and EMR systems are primarily designed to facilitate practices in managing patient health data. However, EHR systems offer a more comprehensive view of such data.
On the other hand, practice management software also streamlines the operational and financial aspects of a practice, focusing on processes including billing and scheduling.
Read More...Physician Fee Schedule Policy Changes: Lookup Medicare PFS Proposed Rule
Posted on November 28th, 2023 / Under Medical Billing / With No Comments
The Medicare physician fee schedule dictates how services rendered by healthcare providers are compensated under the Medicare program for their services.
Centers for Medicare and Medicaid regularly update the physician fee schedule to align with technological changes and concurrent transformations within the healthcare industry.
Some exciting transformations are awaiting the healthcare landscape in the upcoming year and at the forefront lies the 2024 Medicare physicians fee schedule proposed rule.
Similar to the CY 2023 physician fee schedule, the 2024 physician fee schedule proposed rule is aimed at fostering a more equitable healthcare system. Effective implementation of the proposed policy changes will elevate the level of patient care.
Let’s uncover the basics of PFS and what the physician fee schedule final rule 2023 addresses.
Understanding PFS Basics
The world of healthcare finance is filled with intricacies, and the physician fee schedule is one of its cornerstones that every provider must understand thoroughly.
Simply put, a physician fee schedule is defined as a list of fees assigned to different services and procedures healthcare professionals render to patients. These lists are used by insurance providers and Medicare to reimburse physicians and other healthcare providers.
Physicians provide services in various healthcare settings, including hospitals, physicians’ offices, hospices, outpatient dialysis facilities, and clinical laboratories. PFS ensures that the payment rates remain consistent across all healthcare settings.
On the other hand, some payers also use the MPFS (Medicare Physician Fee Schedule) as a reference for reimbursing doctors. The MPFS is an annual rule that specifically outlines and updates reimbursement rates for services doctors render to Medicare beneficiaries.
According to the medicare physician’s fee schedule, procedures are assigned relative value by factoring in relevant practice expenses, liability insurance, and the physician’s work. This value is then multiplied by a conversion factor to derive payment rates.
To account for any regional variations in the cost of operating a practice, further adjustment to the derived value can be made using GPCI (geographic practice code index).
For an accurate reflection of the costs associated with a physician’s work and the technical resources utilized to perform a procedure or service, the professional and technical components of a service can be segregated.
For instance, the professional component of a service indicates activities such as evaluation of a patient, diagnosis, etc, and this component is billed by the assigned physician.
On the other hand, the technical component of a service signifies the use of facilities and equipment to perform technical aspects of a service such as a laboratory test or imaging. Technical components are typically billed by suppliers such as dialysis facilities, radiology centers, and ambulatory surgical centers.
Role of PFS In Medical Billing
The physician fee schedule holds great significance in the world of medical and physician billing, influencing how procedures and services are translated into proper codes, billed by suppliers and practitioners, and reimbursed by payers.
PFS provides a standardized framework for medical services’ reimbursement, contributing to billing transparency. This transparency allows payers to assess the validity of billed charges and for practitioners to comprehend reimbursement rates across different healthcare settings and different types of services.
PFS Payment Rates
The physician fee schedule is typically updated annually, and specific payment rates in PFS can vary depending on various factors, including updates made by CMS, geographical location of practice, and the types of services rendered.
However, there is a standard formula used to determine payment for a service, which is:
Work RVU (relative value units) x Work GPCI (geographic price cost index) + PE (practice expense) RVU x PE GPCI + MP (malpractice) RVU x MP GPCI = Total RVU x CF (conversion factor) = Payment.
Providers can use the medicare physician fee schedule lookup tool to get further insights on billing, coding, and payment rates.
Medicare Physician Fee Schedule Proposed Rule 2024
Here is what you should know about the 2024 medicare physician fee schedule final rule.
- Compared to the conversion rate of $33.58 in the CMS physician fee schedule 2022 and $33.06 in the 2023 medicare physician fee schedule final rule, the final CY 2024 PFS conversion factor was reduced by 1.15% to $32.74.
- In the CY 2024 proposed physician fee schedule, the overall rates will be subject to a reduction of 1.25%.
- CMS has also finalized reimbursement for providers who train other caregivers to assist patients diagnosed with specific illnesses. Payments will be provided as a part of the patient’s individualized treatment plan.
- Effective January 1st, 2024, an additional payment for the new add=on HCPCS code G2211 will be introduced.
- CMS has also finalized the definition for the phrase “substantive portion” used specifically for split/shared E/M visits. The substantive portion now signifies a key element of medical decision-making and more than half of the total time the physician or non-physician practitioner spends performing the split/shared E/M visit.
- On a temporary basis, health and well-being coaching services are being added to the Medicare Telehealth Services list for CY 2024.
- The implementation of the Appropriate Use Criteria (AUC) program has been temporarily put on hold by CMS.
- The 2024 PFS final rule also implements notable changes to the Medicare Shared Savings Program (MSSP).
FAQs
What is the difference between FFS and PFS?
FFS (fee-for-service) is more of a traditional payment model where providers are reimbursed for each service they render. On the other hand, PFS is a component of FFS in which payment rates are based on relative values.
What are the definitions for facility and non-facility for the physician fee schedule?
Facility and non-facility both refer to different payment settings. For instance, a non-facility rate is used for services rendered in non-facility settings like a physician’s office, and facility rates are used for services rendered in hospitals and other healthcare facilities.
Read More...Patient Demographics Documentation Guidelines
Posted on November 27th, 2023 / Under Medical Billing / With No Comments
When a patient enters a healthcare facility to acquire treatment, one of the first things the staff does is collect the patient’s information. That information is called patient demographics.
Sounds straightforward enough, right? Only patient demographics have much more depth to it than just supporting physicians in providing high-quality care.
Patient demographics serve a multifaceted role, addressing several concerns, one of which is payment collection. Demographic data not only informs treatment plans but also ensures billing accuracy.
Lack of accuracy in patient demographic collection can lead to increased cost and duplicate testing, according to AHIMA medical coding and patient demographic standards.
To ensure a smoother medical billing process, let’s dive into what’s included in patient demographics and why it is important.
What Do Patient Demographics Include?
An accurate and complete patient demographic form typically includes all the information that’s required to streamline the medical billing process. Patient demographics can include but are not limited to the following:
- The full legal name of the patient.
- Date of birth.
- Gender of the patient.
- Address and contact information such as phone number and email address.
- Social security number for insurance and billing purposes.
- Insurance information such as policy number, insurance coverage, and name of provider.
- Guarantor information for patients who are minors.
- Emergency contact information.
- Ethnicity and race.
- Marital status.
- Language preference to facilitate effective communication between the patient and the provider.
- Employment status, which can be relevant to insurance information.
Some healthcare providers may consider medical histories such as family medical history, present medical condition, drug or other allergies, and surgical history as non-demographic data and include it only in the patient medical chart, while others may include it in the demographic sheet.
Collecting Patient Demographics Data
Patient demographics are collected during the registration process and are generally digital. Healthcare facilities use EHR systems to capture and store patient demographic data.
Patient demographic forms are also updated and secured through patient portals. The CDI medical process is further implemented by a clinical documentation improvement (CDI) specialist to ensure the accuracy of clinical data.
While this data can be collected in multiple ways, the patient demographic sheet has to meet specific standards, such as being HIPAA-friendly.
If healthcare entities are taking a verbal approach, they should avoid using jargon that could confuse the patients and impact data accuracy. Healthcare professionals should also assure patients that their demographic data will be kept confidential.
While many EHRs are already configured to collect medical documentation, some practices have untrained staff that may not know how to work the system properly, resulting in missing or incomplete patient information.
According to the CMS Medical Record Documentation Guidelines 2022, insufficient medical documentation can allow the reviewer to reject claims, concluding that the billed services were either not provided or were not medically necessary.
The key to a successful collection of patient demographic information is for physicians to train their staff on how to effectively use EHR systems. Having a standard collection process and using advanced software can streamline the process of collecting patient demographics.
Importance of Patient Demographics
Here is why patient demographics are important.
Streamlined Medical Billing Process
One thing that consistently serves as a factor for claim denials is inaccurate and missing patient data. Patient demographic information directly impacts medical billing as it includes some critical information, including whether to bill the primary or secondary insurance provider for the services rendered to the patient.
Without gathering patient demographics, the billing procedure can be significantly delayed. For instance, without collecting such data, it can be difficult to confirm whether a patient without health coverage is eligible to be covered under the charity care program.
Cultural Competence
Patient demographics data such as race, gender, and age can assist you in creating individualized treatment plans for specific patient populations.
It’s essential to improve the cultural competence of your healthcare staff to make your practice an inclusive place where patients from all backgrounds can receive exceptional care.
An in-depth understanding of your patient’s history and cultural background will allow you to provide more personalized treatment to your patients.
Improving Patient Care
Assessing the details of the patient demographics can help you improve patient care by determining risk factors and prescribing effective treatment. Knowing the patient’s medical history will allow physicians to tailor treatment plans to their specific conditions, improving the level of care provided.
Gateway to Effective Patient Communications
One of the benefits of patient demographics is seamless communication between patients and providers. Many healthcare practices offer online portals to help patients update demographic information, such as their contact information, which may change over time.
This leads to a reduction in missed or canceled doctor’s appointments as patients can be reminded effectively. Doctors can also interact with patients better, ensuring they stick to their treatment plans.
FAQs
What are some things to keep in mind for patient demographics?
One thing you should keep in mind when managing patient demographics is that accuracy is paramount. Ensure that you collect all personal details precisely and address diversity and cultural sensitivity in your practice. Safeguard patient privacy and ensure regular updates on medical records to reflect any changes in treatment.
Where does HIPAA factor in?
HIPAA (Health Insurance Portability and Accountability Act) ensures the security and confidentiality of patient information, emphasizing the privacy rights of patients. All healthcare practices are required to comply with HIPAA standards to safeguard against unauthorized access to sensitive patient information.
Read More...A Comprehensive Guide to Telehealth Billing 2023
Posted on October 27th, 2023 / Under Medical Billing / With No Comments
COVID-19 has brought multiple changes into our daily lives; one of those changes is a growing number of people opting for telehealth. Compared to 2019, when only 10% of people actively acquired telehealth services, a recent survey shows that approximately 52% of adults use telemedicine.
Post-pandemic, there was a surge in demand for telehealth services because many patients deem it a more convenient option than in-person visits. Now, approximately 76% of healthcare organizations in the U.S. allow patients to consult with providers virtually.
Telemedicine is significantly different today from what it was pre-pandemic. Even the recent legislation by the U.S. Department of Health and Human Services authorized multiple changes, some of which are permanent.
In this guide, we’ll help you navigate medicare telehealth billing guidelines 2023, including updated telehealth CPT codes, telemedicine modifiers, and reimbursement for telehealth.
Telemedicine is significantly different today from what it was pre-pandemic. Even the recent legislation by the U.S. Department of Health and Human Services authorized multiple changes, some of which are permanent.
In this guide, we’ll help you navigate medicare telehealth billing guidelines 2023, including updated telehealth CPT codes, telemedicine modifiers, and reimbursement for telehealth.
What Is Telehealth?
Telehealth, also known as telemedicine, is a term used to describe the use of telecommunication and electronic information to address health needs. Common technologies to extend care include streaming media, wireless communications, and video conferencing. Telemedicine billing services can vary depending on your geographic location and the insurance provider or payer you are billing.
Benefits of Using Telehealth
One main reason people were using telehealth during COVID-19 is because it eliminated the travel burden for patients who were vulnerable to the virus. Other than that, telehealth provides multiple benefits, including,
- Vital details of a patient’s health can reach their assigned caretakers and healthcare team in time with the help of health monitoring services.
- People struggling with poor mental health can seek online therapy services.
- You can partner with telepharmacy services to deliver prescriptions to your patient’s doorstep.
- With telehealth, uninsured patients are billed by providers at a price similar to a normal insurance copay, expanding their access to healthcare services.
Getting Reimbursed for Telehealth
One common query most providers have is how they will get reimbursement for telehealth. The answer is that reimbursement rates for telehealth can vary due to laws such as the Pay Parity Laws and whether the qualified healthcare professional is receiving reimbursement from a private payer, Medicaid plan, or Medicare.
For instance, if you live in one of the states that follow the pay parity laws, you will get reimbursement for telehealth similar to the reimbursement you get for in-person visits for the respective service.
Telehealth Billing Guidelines 2023
Telehealth Modifier 93
Generally, all telehealth sessions, except audio-only sessions, are billed using the modifier 95 or the GT modifier, varying depending on the payer billed for the services. Modifier 95 description includes the CPT code modifier used to bill telehealth services with the place of service code 11, which indicates an office. The place of service code 11 is the same code used when services are rendered in person.
Modifier 93 is a new CPT code modifier that came into effect at the start of 2022. This modifier describes a real-time interaction between a patient and a qualified healthcare professional located at different sites. It is essential for healthcare providers to bill all audio-only telehealth services using this modifier.
Temporary Changes In Medicare Telehealth 2023
The changes made in the COVID-19 Public Health Emergency (PHE) were initially meant to be temporary, but the bill passed at the end of last year caused these temporary changes in telehealth billing guidelines to be extended through December 31, 2024.
Two temporary changes that ended back in May included telehealth being provided as an exceptional benefit and Medicare-covered providers not being subject to a federal penalty for using applications that aren’t HIPAA-complaint to communicate with their patients.
The changes that will extended through December 2024 are:
- Mental health and non-behavioral services can be obtained at any site. Originating site geographic restrictions for these services are waived.
- Some mental health and non-behavioral services can be delivered through audio-only communication.
- In-person visits within the first six months of initial non-behavioral and mental health service are also not required. The effective date of this rule was postponed for 151 days after the PHE, which ended in May.
- Occupational therapists, pathologists, audiologists, and physical therapists are now considered practitioners who can provide care using telehealth.
Permanent Medicare Telehealth Changes
The focus of the majority of permanent changes made by the CMS (Centers for Medicare and Medicaid) is on mental health care. These include:
- RHCs (Rural Health Clinics) and FQHCs (Federally Qualified Healthcare Centers) can be distant site providers for non-behavioral and mental health services.
- One of the eligible originating sites for telemedicine services is REH (Rural Emergency Hospital).
- Practitioners will no longer receive separate reimbursement for audio-only E/M services.
- Virtual Direct Supervision is set to continue only until the end of 2023 and will not remain a permanent feature of Medicare.
- Although CMS suggested five new codes to be added permanently to the Medicare Telehealth Services list, only three codes for chronic pain management and prolonged E/M services are made permanent as they are sufficiently similar to other services listed currently on a Category 1 basis.
FAQs
How to bill for telemedicine?
To bill for telemedicine, you must first determine the usage and type of telemedicine you offer, check any reimbursement and compliance policies appertaining to your claim, perform accurate coding using modifier 95 or GT depending on the payer, and finally add any CPT codes applicable to the telehealth services rendered.
Is telehealth covered by insurance in 2023?
Other than Medicare and Medicaid, telemedicine services are covered by most private health insurance plans. However, depending on the state you belong to and the insurance carrier’s policies, reimbursement rates and telehealth coverage may vary. Telehealth services can be rendered through online consultations, audio, or video, so it is best to check in with the payer on what they cover and get a clear idea of the billing requirements.
Does Medicare cover telehealth?
Typically, telehealth services are covered under Medicare Part B, which has a deductible of $226 in 2023. So, after a patient meets the part B deductible, they only pay 20% of the total Medicare-approved amount to their assigned physician or healthcare provider for the services rendered.
Read More...Medical Coding Audits: What You Need to Know to Stay Compliant
Posted on October 23rd, 2023 / Under Medical Billing / With No Comments
Effective management of healthcare information is incomplete without medical coding. Coding audits are a critical practice performed by a clinical coding auditor to ensure the practice has proper procedures set in place to achieve medical coding compliance.
Centers for Medicare and Medicaid Services (CMS)and the Office of the Inspector General (OIG) recommend healthcare organizations obtain an unbiased evaluation of their coding practices. This helps providers identify and eliminate errors in medical coding, maintain regulatory compliance, and expedite the reimbursement process.
Keep reading to learn about how medical coding audits can help you avoid major pitfalls stemming from coding errors.
Importance of Medical Coding Audits
Coding reviews include examining the medical records of the patients to ensure the provider has selected and entered correct and comprehensive diagnosis and procedure codes.
A medical records audit generally includes an examination of documentation to ensure it is accurate and complete, reviewing CPT codes, checking the location of patient care, ensuring the modifiers are not absent or incorrect, any absence or presence of any bundling concerns, and a medical coding utilization review.
Research shows that around 80% of medical bills contain some type of coding and billing errors, costing patients an extravagant amount of money compared to the level of service obtained. Other consequences of not conducting regular coding audits include damage to your practice’s reputation, lost revenue, and compliance risks.
Medical coding audits can help you uncover any current problematic trends in your practice, including upcoding, outdated coding, unbundling, and downcoding. For instance, multiple issues can affect medical coding accuracy, such as a lack of documentation. A general rule of thumb is medical coders are only able to use the documentation they are provided, so if a healthcare provider records documentation with missing details, it will lead to medical coding errors. Such errors can be identified through regular coding audits.
Another important reason for organizations to conduct these audits is compliance. Coding and billing practices are required to be in compliance with multiple regulations, including private payer policies, CMS, and OIG regulations. This puts the organization at risk of facing legal repercussions.
Benefits of Regular Medical Coding Audits for a Healthcare Practice
Reduction in Claim Denial
One common reason why most medical claims get denied at the initial stages is coding errors. Some common issues uncovered during these audits include any wrong diagnosis or procedure codes and insufficient documentation. With proper coding audit policy and procedure, coding errors are minimized. This reduces the risk of medical claims getting denied or rejected by the payer’s insurance provider.
Revenue Protection
Coding mistakes are one of the major reasons why healthcare practices incur financial loss. For instance, if a claim is under-coded, there are still chances of it getting processed by the payer; this results in practice losing money by getting reimbursed for less than the actual level of services rendered. On the other hand, over-coded claims put the practice at potential risk of a regulatory fine.
Moreover, coding mistakes discovered during claims processing can cause the payer to deem the claim unpayable. This results in healthcare providers investing extra time and effort into fixing coding mistakes and resubmitting claims. However, with effective medical coding audit software, potential issues can be identified early in the process, helping your organization avoid such revenue loss.
Fraud Reduction
Another reason why periodic medical coding audits are essential is compliance issues and billing fraud. Medical coding audit documents allow organizations to identify any improper billing practices, such as invoicing for services not acquired by the patient or unnecessary services, and help uncover whether such issues were caused through intention or coding error. This allows healthcare organizations to take action and have their staff follow proper billing protocols to eliminate billing fraud.
Coding Accuracy Improvement
The acceptable coding accuracy rate is 95%, and research shows that medical coding accuracy actually falls way beneath this standard. Coding accuracy impacts your risk judgment and quality of reporting. One major factor that affects coding quality is missing or incorrect documentation, which can easily be identified through coding audits.
Educating Your Staff
One of the many benefits of coding audits is medical coding training. These audits allow your staff to improve as a team and ensure that your coders have proper training.
For example, outpatient coding audits will allow your coding team to develop a comprehensive understanding of the CPT system and get informed of the updated regulations. Inpatient coding audits allow coders to recognize changes in AHA (American Hospital Association) guidelines and ICD codes. This way, your coding staff will acquire all the necessary skills required to ensure coding accuracy.
Preventing Payer Audits:
It is possible for your practice to get flagged for investigation by a payer if coding issues become persistent. The purpose of this investigation is to identify potential coding and billing fraud in practice, which, if found, can lead to financial consequences, including hefty fines. Regular audits can help you avoid any payer investigations for waste, abuse, or billing fraud.
Internal and External Coding Audits
Generally, a member of the healthcare staff is employed by the organization to conduct an internal coding audit. This could be the auditing team members in large facilities and a clinical coding auditor in smaller organizations.
Internal coding audits help organizations identify areas of improvement and assess coding accuracy. While it is recommended to conduct regular internal coding audits, the actual frequency of these audits can vary depending on the size of a practice and its available resources.
External coding audits, on the other hand, are conducted by third-party auditing companies or government companies like OIG and are relatively more objective. These audits can take place biannually or even annually in some organizations.
External coding audits play a vital role in identifying recurrent coding errors and fraudulent coding practices within the organization. These audits have more value than internal audits as they are performed by an independent party.
Coding audits, whether external or internal, are essential if your organization wants to maintain medical coding integrity, prevent fraudulent activities, and avoid potential pitfalls.
Read More...Recent Posts
-
False Claims Act Impact On Medical Billing and Coding
Initially, the False Claims Act in healthcare was enacted during the Civil wall to impose liability on individuals and organi...
Read More... -
Role of Encounter Forms in Provider Records and Billing
On average, a doctor wo...
Read More... -
Free Standing Emergency Rooms Billing Services And Your Need To Outsource
Freestanding ER may be a new trend in the healthcare industry, but they have been around for ages. The purpose of freestandin...
Read More... -
Physician Credentialing Importance In Healthcare Improvement
According to a recent survey, Read More...
-
Medicare 8 minute Rule Billing: Also Known As Direct Time CPT Codes
Underbilling is a serious issue in the healthcare industry, and one primary cause is the providers’ lack of knowledge regar...
Read More...
